Protecting Against Calcaneal Spur

Overview
A heel spur is a painful condition that is caused by the accumulation of excessive calcium under the heel of the foot. The heel bone is made up of a large structure called the calcaneus, which is connected to the bottom of the foot by durable connective tissue called fascia. If the layers of connective tissue become damaged or begin to degenerate due to wear and tear, plantar fasciitis may develop. This causes calcification, which refers to the abnormal buildup of calcium on the heel bone. As the calcium continues to accumulate, a calcified protrusion called a spur may become visible on an X-ray.
Causes
One frequent cause of heel spurs is an abnormal motion and mal-alignment of the foot called pronation. For the foot to function properly, a certain degree of pronation is required. This motion is defined as an inward action of the foot, with dropping of the inside arch as one plants the heel and advances the weight distribution to the toes during walking. When foot pronation becomes extreme from the foot turning in and dropping beyond the normal limit, a condition known as excessive pronation creates a mechanical problem in the foot. In some cases the sole or bottom of the foot flattens and becomes unstable because of this excess pronation, especially during critical times of walking and athletic activities. The portion of the plantar fascia attached into the heel bone or calcaneous begins to stretch and pull away from the heel bone.
Symptoms
Heel spurs may or may not cause symptoms. Symptoms are usually related to the plantar fasciitis. You may experience significant pain. Your heel pain may be worse in the morning when you first wake up or during certain activities.
Diagnosis
Diagnosis is made using a few different technologies. X-rays are often used first to ensure there is no fracture or tumor in the region. Then ultrasound is used to check the fascia itself to make sure there is no tear and check the level of scar tissue and damage. Neurosensory testing, a non-painful nerve test, can be used to make sure there is not a local nerve problem if the pain is thought to be nerve related. It is important to remember that one can have a very large heel spur and no plantar fasciitis issues or pain at all, or one can have a great deal of pain and virtually no spur at all.
Non Surgical Treatment
Over-the-counter or prescription-strength anti-inflammatory medications can help temporarily, but can cause side effects with prolonged use - the most significant being gastrointestinal upset, ulceration and bleeding. Deep tissue massage, taping and other physical therapy modalities can also be helpful. Arch support is highly recommended, either with shoe inserts or custom orthotics made by podiatrists. If pain continues, a steroid injection at the site of pain may be recommended; however, many physicians do not like injecting around the heel. The side effects of steroids injected in this area can be serious and worsen symptoms. Complications can include fat necrosis (death of fatty tissue) of the heel and rupture of the plantar fascia.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.
Bursa Foot Surgery Treatment
Overview
This is a very common condition that leads to foot pain . Once you understand what it actually is you will wonder why it does not occur more often, particularly in the foot. It is an inflamed bursal sac. A bursal sac is a sac filled with fluid that acts to lubricate and reduce the friction between two surfaces in the body, usually muscles and tendons as they glide over bony prominences, however their purpose in not limited to just muscles and tendons. The body contains literally hundreds of bursal sacs but in the foot there is just one naturally occurring (adventitious) bursal sac. It is located between the Achilles tendon and the heel bone (calcaneaus), otherwise known as an achilles tendon bursal sac.In this instance the Achilles tendon is protected from the pressure of the heel bone pressing against it when we walk.
Causes
Age. Bursitis is more common during middle age due to repetitive activities that put wear and tear on the body over time. Certain activities or occupations. If your job or hobby involves repetitive motion or puts pressure on bursae, you have a higher likelihood of developing bursitis. Reaching overhead, leaning elbows on arm rests, crossing your legs, laying carpet, setting tile, gardening, biking, playing baseball and ice skating are some activities that, when repeated very often, can put you at increased risk of developing bursitis. Sports in which you may get hit in the knee or fall to the knees, such as football, can also increase the risk. Some medical or health conditions. Rheumatoid arthritis, osteoarthritis, gout, thyroid disease, diabetes, alcoholism and some immunosuppressive disorders can increase the risk of bursitis. The reasons can vary, from cartilage breakdown around joints (arthritis) to crystals in the bursa that cause inflammation (gout). Wearing high heels. Posterior Achilles tendon bursitis occurs when the bursa located between the skin and the Achilles tendon (the band of tissue that attaches the calf muscle to the heel bone) becomes inflamed. High heels are often to blame for this, the stiff heel can put direct pressure on the bursa between the skin and the Achilles tendon.
Symptoms
Pain at the back of the heel, especially with jumping, hopping, tip-toeing, walking or running uphill or on soft surfaces. If tendonitis is also present, the pain can radiate away from the bursa. Direct pressure on the bursa will exacerbate the pain and should be avoided if possible. Tenderness and swelling which might make it difficult to wear certain shoes on the feet. As the bursa becomes more inflamed you will experience swelling and warmth. In severe cases, the bursa will appear as a bump, called a "pump bump", and is usually red, and extremely tender. Swelling can cause difficulties moving as the range of motion in the ankle can be affected. Limping due to the pain may occur. If you press on both sides of the inflamed heel, there may be a firm spongy feeling. Weakness in the tendons and muscles surrounding the bursa can develop as the pain worsens and the inflammation in the area spreads. Possibly a fever if you are suffering from septic bursitis (You will need to see a doctor for medication to get rid of the infection). Pain at the back of the heel makes it difficult to continue wearing shoes, especially high heels with straps or shoes that don't fit properly.
Diagnosis
A physical examination will be performed to determine if you have any signs of Achilles Bursitis or other ankle injury. He/she will look and feel the soft tissue and bones in your ankles to note any differences between the two of them. This will identify any abnormalities, such as swelling, bone deformities, atrophied muscles, redness and/or warmth on the skin. In many cases, the first sign that you have Achilles bursitis is swelling in the back of the foot and ankle pain.
Non Surgical Treatment
With anterior and posterior Achilles tendon bursitis, applying warm or cool compresses to the area and using nonsteroidal anti-inflammatory drugs (NSAIDs) can temporarily relieve the pain and inflammation, as can injections of a corticosteroid/anesthetic mixture into the inflamed bursa. The doctor is careful not to inject the mixture into the tendon. After this treatment, the person should rest. When these treatments are not effective, part of the heel bone may need to be surgically removed.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Prevention
After taking a history and performing a physical examination, your physician may order x-rays to rule out other disorders. Your doctor may administer injections of corticosteroids and a local anesthetic to reduce swelling and ease pain. Also, to reduce swelling, your physician may draw excess fluid from the bursa with a syringe and then tightly wrap and compress the joint with an elastic bandage. In severe, persistent cases surgery to remove the bursa may be necessary. For infectious bursitis, antibiotics will be prescribed.
This is a very common condition that leads to foot pain . Once you understand what it actually is you will wonder why it does not occur more often, particularly in the foot. It is an inflamed bursal sac. A bursal sac is a sac filled with fluid that acts to lubricate and reduce the friction between two surfaces in the body, usually muscles and tendons as they glide over bony prominences, however their purpose in not limited to just muscles and tendons. The body contains literally hundreds of bursal sacs but in the foot there is just one naturally occurring (adventitious) bursal sac. It is located between the Achilles tendon and the heel bone (calcaneaus), otherwise known as an achilles tendon bursal sac.In this instance the Achilles tendon is protected from the pressure of the heel bone pressing against it when we walk.
Causes
Age. Bursitis is more common during middle age due to repetitive activities that put wear and tear on the body over time. Certain activities or occupations. If your job or hobby involves repetitive motion or puts pressure on bursae, you have a higher likelihood of developing bursitis. Reaching overhead, leaning elbows on arm rests, crossing your legs, laying carpet, setting tile, gardening, biking, playing baseball and ice skating are some activities that, when repeated very often, can put you at increased risk of developing bursitis. Sports in which you may get hit in the knee or fall to the knees, such as football, can also increase the risk. Some medical or health conditions. Rheumatoid arthritis, osteoarthritis, gout, thyroid disease, diabetes, alcoholism and some immunosuppressive disorders can increase the risk of bursitis. The reasons can vary, from cartilage breakdown around joints (arthritis) to crystals in the bursa that cause inflammation (gout). Wearing high heels. Posterior Achilles tendon bursitis occurs when the bursa located between the skin and the Achilles tendon (the band of tissue that attaches the calf muscle to the heel bone) becomes inflamed. High heels are often to blame for this, the stiff heel can put direct pressure on the bursa between the skin and the Achilles tendon.
Symptoms
Pain at the back of the heel, especially with jumping, hopping, tip-toeing, walking or running uphill or on soft surfaces. If tendonitis is also present, the pain can radiate away from the bursa. Direct pressure on the bursa will exacerbate the pain and should be avoided if possible. Tenderness and swelling which might make it difficult to wear certain shoes on the feet. As the bursa becomes more inflamed you will experience swelling and warmth. In severe cases, the bursa will appear as a bump, called a "pump bump", and is usually red, and extremely tender. Swelling can cause difficulties moving as the range of motion in the ankle can be affected. Limping due to the pain may occur. If you press on both sides of the inflamed heel, there may be a firm spongy feeling. Weakness in the tendons and muscles surrounding the bursa can develop as the pain worsens and the inflammation in the area spreads. Possibly a fever if you are suffering from septic bursitis (You will need to see a doctor for medication to get rid of the infection). Pain at the back of the heel makes it difficult to continue wearing shoes, especially high heels with straps or shoes that don't fit properly.
Diagnosis
A physical examination will be performed to determine if you have any signs of Achilles Bursitis or other ankle injury. He/she will look and feel the soft tissue and bones in your ankles to note any differences between the two of them. This will identify any abnormalities, such as swelling, bone deformities, atrophied muscles, redness and/or warmth on the skin. In many cases, the first sign that you have Achilles bursitis is swelling in the back of the foot and ankle pain.
Non Surgical Treatment
With anterior and posterior Achilles tendon bursitis, applying warm or cool compresses to the area and using nonsteroidal anti-inflammatory drugs (NSAIDs) can temporarily relieve the pain and inflammation, as can injections of a corticosteroid/anesthetic mixture into the inflamed bursa. The doctor is careful not to inject the mixture into the tendon. After this treatment, the person should rest. When these treatments are not effective, part of the heel bone may need to be surgically removed.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Prevention
After taking a history and performing a physical examination, your physician may order x-rays to rule out other disorders. Your doctor may administer injections of corticosteroids and a local anesthetic to reduce swelling and ease pain. Also, to reduce swelling, your physician may draw excess fluid from the bursa with a syringe and then tightly wrap and compress the joint with an elastic bandage. In severe, persistent cases surgery to remove the bursa may be necessary. For infectious bursitis, antibiotics will be prescribed.
Recuperating From Bunion And Hammertoe Surgery
 Overview
Overview
Hammer toe is most common in women, and a big part of this is poor shoe choices, which are a big factor in the development of many foot problems. Tight toe boxes and high heels are the biggest culprits. Genetics certainly plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. Most cases of contracted toes are associated with various biomechanical abnormalities in how a patient walks. This causes the muscles and tendons to be used excessively or improperly, which deforms the toes over time.
Causes
A common cause of hammer toe is wearing shoes that do not fit properly. Poorly-fitting shoes can hold the toes in an abnormal position and result in tightening of the muscles required to maintain that position. In particular, shoes that have high heels and are narrow at front tend to push the toes into an abnormal, bent position. Less commonly, diseases of the nerves, muscles, or joints (such as arthritis) can result in the hammer toe deformity.
 Symptoms
Symptoms
Some people never have troubles with hammer toes. In fact, some people don't even know they have them. They can become uncomfortable, especially while wearing shoes. Many people who develop symptoms with hammer toes will develop corns, blisters and pain on the top of the toe, where it rubs against the shoe or between the toes, where it rubs against the adjacent toe. You can also develop calluses on the balls of the Hammer toe feet, as well as cramping, aching and an overall fatigue in the foot and leg.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
What will a doctor do? Treat any foot complaints such as corns, calluses by periodically reducing the lesion and applying appropriate pads and dressings. Recommend the silicone toe prop. If an infection is present, then anti-septic dressings, antibiotics and pads to redistribute pressure away from the lesion may be necessary. In the case of a mallet toe, trigger toe or claw toe. If a corn occurs at the end of the toe, a silicone or leather prop may be used to straighten the toe. In a hammertoe deformity, a silicone prop to redistribute pressure away from a corn may be necessary. The doctor may give footwear advice. In severe cases, corrective surgery may be necessary. The doctor may recommend orthosis to correct a mechanical complaint of the foot, such as 3/4 length silicone insoles.
Surgical Treatment
Surgery to correct for a hammertoe may be performed as an outpatient procedure at a hospital, surgery center, or in the office of your podiatrist. There are multiple procedures that can be used depending on your individual foot structure and whether the deformity is flexible or rigid. There may be a surgical cut in the bone to get rid of an exostosis, or a joint may be completely removed to allow the toe to lay straight.
Contracted Toe Treatment
 Overview
Overview
A hammertoe is a deformity in the foot, causing the second, third, or fourth toe to be permanently bent in the middle joint, causing the toe to resemble a hammer (hence, its name!) or a claw. They are most commonly found in women who wear narrow shoes, such as high heels, that cause the toes to bend unnaturally for extended periods of time. A hammertoes may be difficult or painful to move, and the skin may become callused from rubbing against the inside of the shoe. In fact, there are two types of hammertoe: flexible and rigid. Flexible hammertoes can still move at the joint and are indicative of hammertoes an earlier, milder form of the problem. Rigid hammertoes occur when the tendon no longer moves, and at this stage, surgery is usually necessary to fix the problem.
Causes
But what causes the imbalance of the tendons and muscles in the first place so that they begin to pull and bend the joint? A bad fitting shoe could be the cause but it usually isn?t the primary cause. Many people are genetically predisposed to hammertoe, and the condition begins to progress more quickly when they wear shoes that fit poorly, for example pointy toes, high heels, or shoes that are too short. Hammertoe may also be caused by damage to the joint as a result of trauma.
 Symptoms
Symptoms
A toe stuck in an upside-down "V" is probably a hammertoe. Some symptoms are, pain at the top of the bent toe when putting on a shoe. Corns forming on the top of the toe joint. The toe joint swelling and taking on an angry red colour. Difficulty in moving the toe joint and pain when you try to so. Pain on the ball of the foot under the bent toe. Seek medical advice if your feet regularly hurt, you should see a doctor or podiatrist. If you have a hammertoe, you probably need medical attention. Ask your doctor for a referral to a podiatrist or foot surgeon. Act now, before the problem gets worse.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
The treatment options vary with the type and severity of each hammertoe, although identifying the deformity early in its development is important to avoid surgery. Podiatric medical attention should be sought at the first indication of pain and discomfort because, if left untreated, hammertoes tend to become rigid, making a nonsurgical treatment less of an option. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Surgical Treatment
Surgical correction is necessary in more severe cases and may consist of removing a bone spur (exostectomy) removing the enlarged bone and straightening the toe (arthroplasty), sometimes with internal fixation using a pin to realign the toe; shortening a long metatarsal bone (osteotomy) fusing the toe joint and then straightening the toe (arthrodesis) or simple tendon lengthening and capsule release in milder, flexible hammertoes (tenotomy and capsulotomy). The procedure chosen depends in part on how flexible the hammertoe is.
Bunions And Symptoms
Overview
 A bunion forms when the bursa (a sac of fluid at friction points between the tendons and bone in some areas and between bone and the skin in others) becomes inflamed along the edge of the joint at the base of the big toe. There are two types of bunions. The acute bunion causes the sharper pain. It develops from a bursitis, a sudden outcropping of a fluid-filled sac. An acute bunion can progress into the second type of bunion, the hallux valgus, a chronic but often painless deformity involving permanent rigidity of the bones. Bunions can form in any part of the foot but occur most often at the big toe joint, where the first metatarsal bone abuts the proximal phalanx of the big toe. Women are more likely than men to get bunions because of the misshapen footwear and elevated heels they wear.
A bunion forms when the bursa (a sac of fluid at friction points between the tendons and bone in some areas and between bone and the skin in others) becomes inflamed along the edge of the joint at the base of the big toe. There are two types of bunions. The acute bunion causes the sharper pain. It develops from a bursitis, a sudden outcropping of a fluid-filled sac. An acute bunion can progress into the second type of bunion, the hallux valgus, a chronic but often painless deformity involving permanent rigidity of the bones. Bunions can form in any part of the foot but occur most often at the big toe joint, where the first metatarsal bone abuts the proximal phalanx of the big toe. Women are more likely than men to get bunions because of the misshapen footwear and elevated heels they wear.
Causes
It is thought that the primary cause of bunions is a mechanical instability in the big toe joint. There are a number of different reasons as to why this may happen. Bunions tend to run in families so a person with a family history of bunions has an increased risk of developing them. Factors that are known to increase the risk of bunions include wearing improperly fitting shoes (particularly narrow and/or high-heeled shoes). Certain arthritic conditions and ligament disorders. Age (the incidence of bunions increases with age). Being flatfooted with feet that roll inwards (over pronation). Past injury (trauma) to the foot. Nerve conditions affecting the foot. Bunions most commonly affect women (approximately 90% of cases) and are less common in people who do not regularly wear shoes.
Symptoms
If a foot bunion is developing, you may experience some of these symptoms. Bulge or bump on the outside of the base of your big toe. Swelling. Redness. Soreness. Thickening of the skin in that location. Corns or calluses. Limited movement of your big toe. Persistent or periodic pain. The pain you experience may be mild or severe. It may become increasingly difficult to walk in your normal shoes. The pressure on your other toes can cause your toenails to grow inward or your smaller toes to become bent.
Diagnosis
X-rays are the best way to determine the amount of deformity of the MTP joint. Blood work may be required to rule out other diseases that may be associated with bunions such as rheumatoid arthritis. Other tests such as bone scans or MRI's are not usually required.
Non Surgical Treatment
Bunion treatment should always start with changing footwear to relieve symptoms and to prevent the bunion from progressing. Shoes with a wide toe-box, minimal slope, and good arch support can help relieve the bunion pain. Some people find that ice application and anti-inflammatory medications can help relieve the inflammation around the bunion. 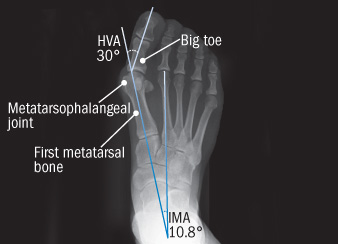
Surgical Treatment
Bunion surgery is most often a day case or one night in hospital. Surgery can be done under ankle block (patient awake) or general anaesthetic. It is best to rest with the foot elevated for the first 2 weeks after surgery. The foot is bandaged and a special sandal supplied by the hospital is worn for 6 weeks. Sensible shoes are to be worn for a further 6 weeks after the bandages are removed. It will take between 3-6 months for the swelling to go down. It will take 12 months before everything completely settles. It is also important to remember that not all bunion operations are entirely successful.
Overpronation Of The Foot
Overview
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Severs Disease In Adolescents
Overview
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
The most common of the Sever?s disease causes is when the heel bone grows more rapidly than the muscles and tendons in the leg. The muscles and tendons become tight and put additional stress on the growth plate in the heel. When this happens, the growth plate begins to swell, becomes tender, and the child will essentially begin to feel one or more Sever?s disease symptoms. It can occur in any child as they grow, but there are some common Sever?s disease causes and risk factors that make a child more prone to the condition. They include participation in sports and other activities that put pressure on the heel, such as basketball, track, and gymnastics. A pronated foot, which makes the Achilles tendon tight, increasing the strain on the growth plate of the heel. An arch that is flat or high, affecting the angle of the heel. Short leg syndrome, when one leg is shorter than the other, causing the shorter leg to pull more on the Achilles tendon in order to reach the ground. Obesity puts extra weight on the growth plate, which can cause it to swell.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
The most common of the Sever?s disease causes is when the heel bone grows more rapidly than the muscles and tendons in the leg. The muscles and tendons become tight and put additional stress on the growth plate in the heel. When this happens, the growth plate begins to swell, becomes tender, and the child will essentially begin to feel one or more Sever?s disease symptoms. It can occur in any child as they grow, but there are some common Sever?s disease causes and risk factors that make a child more prone to the condition. They include participation in sports and other activities that put pressure on the heel, such as basketball, track, and gymnastics. A pronated foot, which makes the Achilles tendon tight, increasing the strain on the growth plate of the heel. An arch that is flat or high, affecting the angle of the heel. Short leg syndrome, when one leg is shorter than the other, causing the shorter leg to pull more on the Achilles tendon in order to reach the ground. Obesity puts extra weight on the growth plate, which can cause it to swell.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.