Bunions And Symptoms
Overview
 A bunion forms when the bursa (a sac of fluid at friction points between the tendons and bone in some areas and between bone and the skin in others) becomes inflamed along the edge of the joint at the base of the big toe. There are two types of bunions. The acute bunion causes the sharper pain. It develops from a bursitis, a sudden outcropping of a fluid-filled sac. An acute bunion can progress into the second type of bunion, the hallux valgus, a chronic but often painless deformity involving permanent rigidity of the bones. Bunions can form in any part of the foot but occur most often at the big toe joint, where the first metatarsal bone abuts the proximal phalanx of the big toe. Women are more likely than men to get bunions because of the misshapen footwear and elevated heels they wear.
A bunion forms when the bursa (a sac of fluid at friction points between the tendons and bone in some areas and between bone and the skin in others) becomes inflamed along the edge of the joint at the base of the big toe. There are two types of bunions. The acute bunion causes the sharper pain. It develops from a bursitis, a sudden outcropping of a fluid-filled sac. An acute bunion can progress into the second type of bunion, the hallux valgus, a chronic but often painless deformity involving permanent rigidity of the bones. Bunions can form in any part of the foot but occur most often at the big toe joint, where the first metatarsal bone abuts the proximal phalanx of the big toe. Women are more likely than men to get bunions because of the misshapen footwear and elevated heels they wear.
Causes
It is thought that the primary cause of bunions is a mechanical instability in the big toe joint. There are a number of different reasons as to why this may happen. Bunions tend to run in families so a person with a family history of bunions has an increased risk of developing them. Factors that are known to increase the risk of bunions include wearing improperly fitting shoes (particularly narrow and/or high-heeled shoes). Certain arthritic conditions and ligament disorders. Age (the incidence of bunions increases with age). Being flatfooted with feet that roll inwards (over pronation). Past injury (trauma) to the foot. Nerve conditions affecting the foot. Bunions most commonly affect women (approximately 90% of cases) and are less common in people who do not regularly wear shoes.
Symptoms
If a foot bunion is developing, you may experience some of these symptoms. Bulge or bump on the outside of the base of your big toe. Swelling. Redness. Soreness. Thickening of the skin in that location. Corns or calluses. Limited movement of your big toe. Persistent or periodic pain. The pain you experience may be mild or severe. It may become increasingly difficult to walk in your normal shoes. The pressure on your other toes can cause your toenails to grow inward or your smaller toes to become bent.
Diagnosis
X-rays are the best way to determine the amount of deformity of the MTP joint. Blood work may be required to rule out other diseases that may be associated with bunions such as rheumatoid arthritis. Other tests such as bone scans or MRI's are not usually required.
Non Surgical Treatment
Bunion treatment should always start with changing footwear to relieve symptoms and to prevent the bunion from progressing. Shoes with a wide toe-box, minimal slope, and good arch support can help relieve the bunion pain. Some people find that ice application and anti-inflammatory medications can help relieve the inflammation around the bunion. 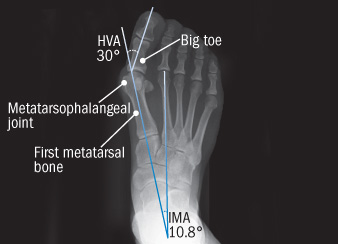
Surgical Treatment
Bunion surgery is most often a day case or one night in hospital. Surgery can be done under ankle block (patient awake) or general anaesthetic. It is best to rest with the foot elevated for the first 2 weeks after surgery. The foot is bandaged and a special sandal supplied by the hospital is worn for 6 weeks. Sensible shoes are to be worn for a further 6 weeks after the bandages are removed. It will take between 3-6 months for the swelling to go down. It will take 12 months before everything completely settles. It is also important to remember that not all bunion operations are entirely successful.
Overpronation Of The Foot
Overview
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
It is important to identify the cause of overpronation in order to determine the best treatment methods to adopt. Not all treatments and preventative measures will work equally well for everyone, and there may be a little trial and error involved to get the best treatment. A trip to a podiatrist or a sports therapist will help you to establish the cause of overpronation, and they will be able to tell you the best treatments based on your specific degree of overpronation and the cause. Overpronation has many causes, with the most common reasons for excessive pronation listed, low arches, flexible flat feet, fallen arches, gait abnormalities, abnormal bone structure, abnormal musculature, bunions, corns and calluses.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Severs Disease In Adolescents
Overview
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
The most common of the Sever?s disease causes is when the heel bone grows more rapidly than the muscles and tendons in the leg. The muscles and tendons become tight and put additional stress on the growth plate in the heel. When this happens, the growth plate begins to swell, becomes tender, and the child will essentially begin to feel one or more Sever?s disease symptoms. It can occur in any child as they grow, but there are some common Sever?s disease causes and risk factors that make a child more prone to the condition. They include participation in sports and other activities that put pressure on the heel, such as basketball, track, and gymnastics. A pronated foot, which makes the Achilles tendon tight, increasing the strain on the growth plate of the heel. An arch that is flat or high, affecting the angle of the heel. Short leg syndrome, when one leg is shorter than the other, causing the shorter leg to pull more on the Achilles tendon in order to reach the ground. Obesity puts extra weight on the growth plate, which can cause it to swell.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
The most common of the Sever?s disease causes is when the heel bone grows more rapidly than the muscles and tendons in the leg. The muscles and tendons become tight and put additional stress on the growth plate in the heel. When this happens, the growth plate begins to swell, becomes tender, and the child will essentially begin to feel one or more Sever?s disease symptoms. It can occur in any child as they grow, but there are some common Sever?s disease causes and risk factors that make a child more prone to the condition. They include participation in sports and other activities that put pressure on the heel, such as basketball, track, and gymnastics. A pronated foot, which makes the Achilles tendon tight, increasing the strain on the growth plate of the heel. An arch that is flat or high, affecting the angle of the heel. Short leg syndrome, when one leg is shorter than the other, causing the shorter leg to pull more on the Achilles tendon in order to reach the ground. Obesity puts extra weight on the growth plate, which can cause it to swell.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Posterior Tibial Tendon Dysfunction Surgery Recovery Time
Overview
Posterior tibial tendon dysfunction is one of several terms to describe a painful, progressive flatfoot deformity in adults. Other terms include posterior tibial tendon insufficiency and adult acquired flatfoot. The term adult acquired flatfoot is more appropriate because it allows a broader recognition of causative factors, not only limited to the posterior tibial tendon, an event where the posterior tibial tendon looses strength and function. The adult acquired flatfoot is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Clinicians need to recognize the early stage of this syndrome which includes pain, swelling, tendonitis and disability. The musculoskeletal portion of the clinical exam can help determine the stage of the disease. It is important to palpate the posterior tibial tendon and test its muscle strength. This is tested by asking patient to plantarflex and invert the foot. Joint range of motion is should be assessed as well. Stiffness of the joints may indicate longstanding disease causing a rigid deformity. A weightbearing examination should be performed as well. A complete absence of the medial longitudinal arch is often seen. In later stages the head of the talus bone projects outward to the point of a large "lump" in the arch. Observing the patient's feet from behind shows a significant valgus rotation of the heel. From behind, the "too many toes" sign may be seen as well. This is when there is abducution of the forefoot in the transverse plane allowing the toes to be seen from behind. Dysfunction of the posterior tibial tendon can be assessed by asking the patient to stand on his/her toes on the affected foot. If they are unable to, this indicates the disease is in a more advanced stage with the tendon possibly completely ruptured.
Non surgical Treatment
Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases. 
Surgical Treatment
If cast immobilization fails, surgery is the next alternative. Treatment goals include eliminating pain, halting deformity progression and improving mobility. Subtalar Arthroereisis, 15 minute outpatient procedure, may correct flexible flatfoot deformity (hyperpronation). The procedure involves placing an implant under the ankle joint (sinus tarsi) to prevent abnormal motion. Very little recovery time is required and it is completely reversible if necessary. Ask your Dallas foot doctor for more information about this exciting treatment possibility.
Managing With Arch Pain
Overview
Arch pain is the term used to describe pin under the arch of the foot. Arch pain is common in people with flat feet. When this occurs it means the person has some inflammation in the mid foot. The arch is supported by a tight band of tissue called the Planter fascia, running from the toes to the heel bone. When this is inflamed it is known as Plantar Fasciitis.

Causes
Often, tarsal tunnel syndrome is misdiagnosed and confused with plantar fasciitis. Tarsal tunnel syndrome is when the tibial nerve which runs through the ankle, is pinched as it passes through the flexor retinaculum, the supportive band that surrounds the ankle joint. The symptoms of tarsal tunnel syndrome are often limited to the ankle but the since the nerve passes through the entire foot it can cause arch pain. Arch pain associated with foot strain is mainly caused by a pronated foot (rolls inward) or a flat foot. These are usually not singular causes of arch pain, but in combination with other factors, arch pain may result.
Symptoms
The groups of muscles that support the arch can be divided into two groups. The muscles on the top of the arch start on the front lower leg and help to lift the arch, and the muscles that help pull the arch on the bottom of the foot are located the on back of the lower leg. Muscle injury may be indicated when pain is felt when the foot is fully extended, flexed, or turned in or out. Pain may also be felt when working the foot against resistance. Bruises are the result of a direct-force injury to the body. A bruise can occur to the foot by a variety of causes, such as having your foot stepped on or by stepping on a rock. The tissues that compose the arch do not provide that area of the body much protection. Blows to the foot that result in pain, discoloration, swelling, and changes in how you walk may indicate more serious damage.
Diagnosis
The diagnosis of high arch (cavus) foot deformity or Charcot Marie Tooth disease can be made by an orthopedic surgeon in the office. Evaluation includes a thorough history and physical examination as well as imaging studies such as X-rays. The orthopedic surgeon will look at the overall shape, flexibility, and strength of a patient?s foot and ankle to help determine the best treatment. Nerve tests may occasionally need to be performed to help confirm the diagnosis.
Non Surgical Treatment
The initial treatment for arch pain, especially if it is of sudden onset is the use of ice to reduce the swelling. Later heat and anti-inflammatory gels can be a big help. Activity should be modified, if you stand a lot at work, see if you can using seating more, if you run a lot, consider swimming or cycling for a while. Use footwear that is supportive in the midfoot and heel area.

Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Stretching Exercises
Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Arch pain is the term used to describe pin under the arch of the foot. Arch pain is common in people with flat feet. When this occurs it means the person has some inflammation in the mid foot. The arch is supported by a tight band of tissue called the Planter fascia, running from the toes to the heel bone. When this is inflamed it is known as Plantar Fasciitis.
Causes
Often, tarsal tunnel syndrome is misdiagnosed and confused with plantar fasciitis. Tarsal tunnel syndrome is when the tibial nerve which runs through the ankle, is pinched as it passes through the flexor retinaculum, the supportive band that surrounds the ankle joint. The symptoms of tarsal tunnel syndrome are often limited to the ankle but the since the nerve passes through the entire foot it can cause arch pain. Arch pain associated with foot strain is mainly caused by a pronated foot (rolls inward) or a flat foot. These are usually not singular causes of arch pain, but in combination with other factors, arch pain may result.
Symptoms
The groups of muscles that support the arch can be divided into two groups. The muscles on the top of the arch start on the front lower leg and help to lift the arch, and the muscles that help pull the arch on the bottom of the foot are located the on back of the lower leg. Muscle injury may be indicated when pain is felt when the foot is fully extended, flexed, or turned in or out. Pain may also be felt when working the foot against resistance. Bruises are the result of a direct-force injury to the body. A bruise can occur to the foot by a variety of causes, such as having your foot stepped on or by stepping on a rock. The tissues that compose the arch do not provide that area of the body much protection. Blows to the foot that result in pain, discoloration, swelling, and changes in how you walk may indicate more serious damage.
Diagnosis
The diagnosis of high arch (cavus) foot deformity or Charcot Marie Tooth disease can be made by an orthopedic surgeon in the office. Evaluation includes a thorough history and physical examination as well as imaging studies such as X-rays. The orthopedic surgeon will look at the overall shape, flexibility, and strength of a patient?s foot and ankle to help determine the best treatment. Nerve tests may occasionally need to be performed to help confirm the diagnosis.
Non Surgical Treatment
The initial treatment for arch pain, especially if it is of sudden onset is the use of ice to reduce the swelling. Later heat and anti-inflammatory gels can be a big help. Activity should be modified, if you stand a lot at work, see if you can using seating more, if you run a lot, consider swimming or cycling for a while. Use footwear that is supportive in the midfoot and heel area.
Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Stretching Exercises
Plantar Fasciitis stretches should always be gentle and pain free, if discomfort occurs with or after stretching decrease the intensity and duration of stretches. Stretches can usually be gradually progressed in intensity and duration over time according to individual tolerance. Plantar Fasciitis Stretch 1. Stretch for the right calf muscle (gastrocnemius) and the arch of the right foot (plantar fascia and muscles under the arches). Take your right heel close to the wall and ball of the foot upright against the wall. Move your hips forwards to the wall. Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 2. Stretch for the outside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot outwards to 2 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the left). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 3. Stretch for the inside belly of the right calf muscle and the arch of the right foot. Take your right heel close to the wall. Turn the ball of your right foot inwards to 10 o?clock position upright against the wall. Move your hips forwards to the wall. Turn your trunk in the opposite direction (i.e. to the right). Try to keep your right leg straight. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times. Plantar Fasciitis Stretch 4. Stretch for the right achilles tendon and the arch of the right foot. Take your right heel close to the wall and ball of the foot upright against the wall (as for stretch 1). Move your hips forwards to the wall. Bend your right knee forwards into the wall keeping the ball of your foot upright against the wall. Push down through your right heel to increase the stretch. Maintain for 30 seconds, repeat 2-3 times.
Acquired Flat Foot Surgery
Overview
Dysfunction of the tibialis posterior tendon is a common condition and a common cause of acquired flatfoot deformity in adults. Women older than 40 are most at risk. Patients present with pain and swelling of the medial hindfoot. Patients may also report a change in the shape of the foot or flattening of the foot. The foot develops a valgus heel (the heel rotates laterally when observed from behind), a flattened longitudinal arch, and an abducted forefoot. Conservative treatment includes non-steroidal anti-inflammatory drugs, rest, and immobilisation for acute inflammation; and orthoses to control the more chronic symptoms. Surgical treatment in the early stages is hindfoot osteotomy combined with tendon transfer. Arthrodesis of the hindfoot, and occasionally the ankle, is required in the surgical treatment of the later stages of tibialis posterior dysfunction. 
Causes
There are a number of theories as to why the tendon becomes inflamed and stops working. It may be related to the poor blood supply within the tendon. Increasing age, inflammatory arthritis, diabetes and obesity have been found to be causes.
Symptoms
Symptoms are minor and may go unnoticed, Pain dominates, rather than deformity. Minor swelling may be visible along the course of the tendon. Pain and swelling along the course of the tendon. Visible decrease in arch height. Aduction of the forefoot on rearfoot. Subluxed tali and navicular joints. Deformation at this point is still flexible. Considerable deformity and weakness. Significant pain. Arthritic changes in the tarsal joints. Deformation at this point is rigid.
Diagnosis
Clinicians need to recognize the early stage of this syndrome which includes pain, swelling, tendonitis and disability. The musculoskeletal portion of the clinical exam can help determine the stage of the disease. It is important to palpate the posterior tibial tendon and test its muscle strength. This is tested by asking patient to plantarflex and invert the foot. Joint range of motion is should be assessed as well. Stiffness of the joints may indicate longstanding disease causing a rigid deformity. A weightbearing examination should be performed as well. A complete absence of the medial longitudinal arch is often seen. In later stages the head of the talus bone projects outward to the point of a large "lump" in the arch. Observing the patient's feet from behind shows a significant valgus rotation of the heel. From behind, the "too many toes" sign may be seen as well. This is when there is abducution of the forefoot in the transverse plane allowing the toes to be seen from behind. Dysfunction of the posterior tibial tendon can be assessed by asking the patient to stand on his/her toes on the affected foot. If they are unable to, this indicates the disease is in a more advanced stage with the tendon possibly completely ruptured.
Non surgical Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful. General components of the treatment include the use of comfort shoes. Activity modification to avoid exacerbating activities. Weight loss if indicated. Specific components of treatment that over time can lead to marked improvement in symptoms include a high repetition, low resistance strengthening program. Appropriate bracing or a medial longitudinal arch support. If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon complex can be successful. In stage 2 deformities, this is combined with an ankle brace for a period of 2-3 months until the symptoms resolve. At this point, the patient is transitioned to an orthotic insert which may help to support the arch. In patients with stage 1 deformity it may be possible to use an arch support immediately. 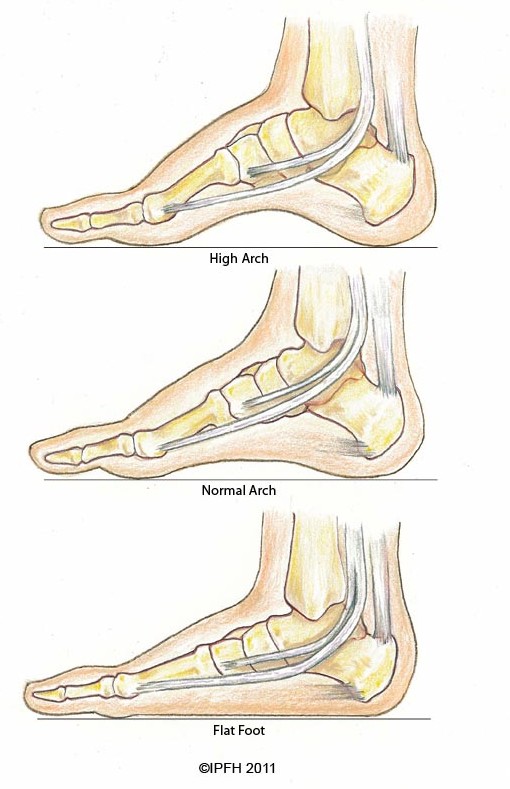
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.
Calf Stretches For Achilles Tendinitis
Overview
 Inflammation of the Achilles tendon.The Achilles is the large tendon connecting the two major calf muscles, gastrocnemius and soleus, to the back of the heel bone. Under too much stress, the tendon tightens and is forced to work too hard. This causes it to become inflamed (that is tendinitis), and, over time, can produce a covering of scar tissue, which is less flexible than the tendon. If the inflamed Achilles continues to be stressed, it can tear or rupture.
Inflammation of the Achilles tendon.The Achilles is the large tendon connecting the two major calf muscles, gastrocnemius and soleus, to the back of the heel bone. Under too much stress, the tendon tightens and is forced to work too hard. This causes it to become inflamed (that is tendinitis), and, over time, can produce a covering of scar tissue, which is less flexible than the tendon. If the inflamed Achilles continues to be stressed, it can tear or rupture.
Causes
The cause of paratenonitis is not well understood although there is a correlation with a recent increase in the intensity of running or jumping workouts. It can be associated with repetitive activities which overload the tendon structure, postural problems such as flatfoot or high-arched foot, or footwear and training issues such as running on uneven or excessively hard ground or running on slanted surfaces. Tendinosis is also associated with the aging process.
Symptoms
The main complaint associated with Achilles tendonitis is pain behind the heel. The pain is often most prominent in an area about 2-4 centimeters above where the tendon attaches to the heel. In this location, called the watershed zone of the tendon, the blood supply to the tendon makes this area particularly susceptible. Patients with Achilles tendonitis usually experience the most significant pain after periods of inactivity. Therefore patients tend to experience pain after first walking in the morning and when getting up after sitting for long periods of time. Patients will also experience pain while participating in activities, such as when running or jumping. Achilles tendonitis pain associated with exercise is most significant when pushing off or jumping.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Nonsurgical methods include rest and stop doing activities that cause stress to the tendon. Ice the area by applying ice to the tendon for 15 minutes after exercising. Compress the tendon by using an athletic wrap or surgical tape. Elevate your injury. You can reduce swelling by lying down and raising your foot at a level that is above your heart. Stretch your ankles and calf muscles. Take anti-inflammatory medication (e.g.: ibuprofen to reduce swelling). Wear orthotics and running shoes. Take part in physical therapy.

Surgical Treatment
Surgical treatment for tendons that fail to respond to conservative treatment can involve several procedures, all of which are designed to irritate the tendon and initiate a chemically mediated healing response. These procedures range from more simple procedures such as percutaneous tenotomy61 to open procedures and removal of tendon pathology. Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months. Open surgery for Achilles tendinopathy has shown that the outcomes are better for those tendons without a focal lesion compared with those with a focal area of tendinopathy.62 At 7 months after surgery, 67% had returned to physical activity, 88% from the no-lesion group and 50% from the group with a focal lesion.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, icorporate stretching into your warm-up and cool-down routines. Maintaining an adequate level of fitness for your sport. Avoid dramatic increases in sports training. If you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse. Wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses. Avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury. Maintain a normal healthy weight.
Inflammation of the Achilles tendon.The Achilles is the large tendon connecting the two major calf muscles, gastrocnemius and soleus, to the back of the heel bone. Under too much stress, the tendon tightens and is forced to work too hard. This causes it to become inflamed (that is tendinitis), and, over time, can produce a covering of scar tissue, which is less flexible than the tendon. If the inflamed Achilles continues to be stressed, it can tear or rupture.
Causes
The cause of paratenonitis is not well understood although there is a correlation with a recent increase in the intensity of running or jumping workouts. It can be associated with repetitive activities which overload the tendon structure, postural problems such as flatfoot or high-arched foot, or footwear and training issues such as running on uneven or excessively hard ground or running on slanted surfaces. Tendinosis is also associated with the aging process.
Symptoms
The main complaint associated with Achilles tendonitis is pain behind the heel. The pain is often most prominent in an area about 2-4 centimeters above where the tendon attaches to the heel. In this location, called the watershed zone of the tendon, the blood supply to the tendon makes this area particularly susceptible. Patients with Achilles tendonitis usually experience the most significant pain after periods of inactivity. Therefore patients tend to experience pain after first walking in the morning and when getting up after sitting for long periods of time. Patients will also experience pain while participating in activities, such as when running or jumping. Achilles tendonitis pain associated with exercise is most significant when pushing off or jumping.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
Nonsurgical methods include rest and stop doing activities that cause stress to the tendon. Ice the area by applying ice to the tendon for 15 minutes after exercising. Compress the tendon by using an athletic wrap or surgical tape. Elevate your injury. You can reduce swelling by lying down and raising your foot at a level that is above your heart. Stretch your ankles and calf muscles. Take anti-inflammatory medication (e.g.: ibuprofen to reduce swelling). Wear orthotics and running shoes. Take part in physical therapy.
Surgical Treatment
Surgical treatment for tendons that fail to respond to conservative treatment can involve several procedures, all of which are designed to irritate the tendon and initiate a chemically mediated healing response. These procedures range from more simple procedures such as percutaneous tenotomy61 to open procedures and removal of tendon pathology. Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months. Open surgery for Achilles tendinopathy has shown that the outcomes are better for those tendons without a focal lesion compared with those with a focal area of tendinopathy.62 At 7 months after surgery, 67% had returned to physical activity, 88% from the no-lesion group and 50% from the group with a focal lesion.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, icorporate stretching into your warm-up and cool-down routines. Maintaining an adequate level of fitness for your sport. Avoid dramatic increases in sports training. If you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse. Wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses. Avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury. Maintain a normal healthy weight.